Disorders of the pituitary may arise when there is overproduction or underproduction of a specific hormone. We will discuss the various disorders that occur due to irregularities in pituitary hormone production. The following disorders will be discussed: hyperpituitarism (acromegaly & gigantism), panhypopituitarism and hypopituitarism, dwarfism, diabetes insipidus (DI), and syndrome of inappropriate antidiuretic hormone (SIADH).
Hyperpituitarism (Acromegaly)
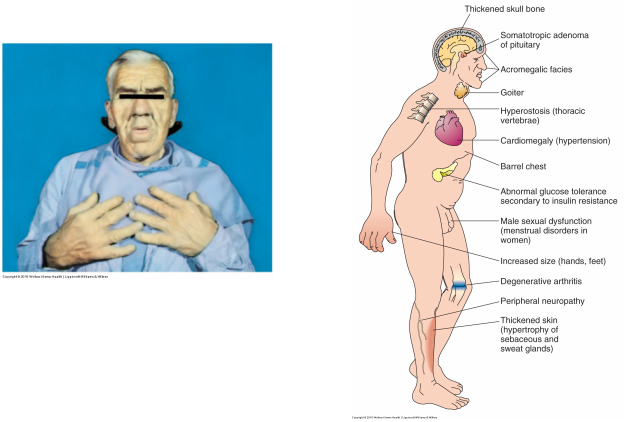
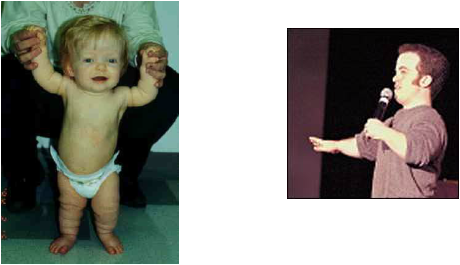
Figure 50-1 (left) and Figure 50-2 (right) Timby & Smith, 2013, p. 757
Pathophysiology and Etiology
Hyperpituitarism is the hyper function of the anterior pituitary gland leading to oversecretion of one of more of anterior pituitary hormones . There is overproduction of the GH, which is usually due to a benign pituitary adenoma, which causes gigantism or acromegaly characterized by bone over growth. This occurs after the epiphyses of the long bones have sealed (acromegaly) (Timby & Smith, 2013, p. 756). Both genders are affected equally. The condition is usually discovered in the teenage years, and surgical or hormone therapy can be prescribed. When it occurs in later years, it is usually the result of an injury to the pituitary gland, such as a car accident. It is a rare, abnormality (approx. 250 people in US are diagnosed each year) that is caused by GH excess.
GH will allow for sustained production of IGF-1 if not checked, and will lead to lengthening and widening of bones, organ enlargement, increased blood glucose levels, and hyperlipidemia (p. 757). The major risk in acromegaly is that the thickening of the bones and cartilage can restrict the function of the heart, lungs and other organs.
Assessment Findings
Diagnostic Findings
ocreotide (Sandostatin), lanreotide (Somutaline), or pegvisomant (Somavert).
Review page 758 in Timby & Smith for information on these drugs.
Hyperpituitarism is the hyper function of the anterior pituitary gland leading to oversecretion of one of more of anterior pituitary hormones . There is overproduction of the GH, which is usually due to a benign pituitary adenoma, which causes gigantism or acromegaly characterized by bone over growth. This occurs after the epiphyses of the long bones have sealed (acromegaly) (Timby & Smith, 2013, p. 756). Both genders are affected equally. The condition is usually discovered in the teenage years, and surgical or hormone therapy can be prescribed. When it occurs in later years, it is usually the result of an injury to the pituitary gland, such as a car accident. It is a rare, abnormality (approx. 250 people in US are diagnosed each year) that is caused by GH excess.
- When excessive secretion occurs before the bones mature = gigantism results
- When excessive secretion occurs after bone maturation= acromegaly
- IGF-1, a hormone released by the liver, stimulates growth of bones and tissue
GH will allow for sustained production of IGF-1 if not checked, and will lead to lengthening and widening of bones, organ enlargement, increased blood glucose levels, and hyperlipidemia (p. 757). The major risk in acromegaly is that the thickening of the bones and cartilage can restrict the function of the heart, lungs and other organs.
Assessment Findings
- Bones increase in thickness and width
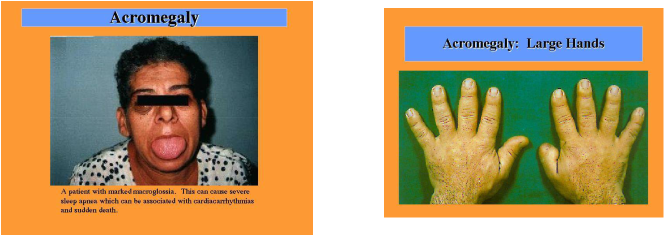
- Physical features include enlargement of hands, feet, and paranasal and frontal sinuses; and deformities of the spine and mandible (jaw protrudes)
- In addition, enlargement of soft tissue (tongue, skin, abdominal organs) causes manifestation such as
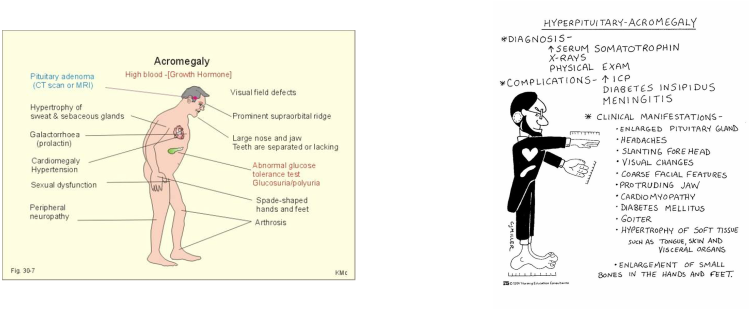
speech difficulties, coarsening of facial features, and abdominal distention - Persons with acromegaly may exhibit deepened voice, increased hair growth, HA, visual problems, diaphoresis, oily, rough skin, peripheral neuropathy, joint pain, and impotence as well as amenorrhea. Some even develop diabetes mellitus.
Diagnostic Findings
- Diagnosed based on history, clinical manifestations, CT, MRI, cranial x-ray, labs revealing serum GH levels and
glucose levels from glucose tolerance tests are most reliable method to confirm acromegaly. Glucose should lower GH levels but in acromegaly GH levels remain elevated.
- Treatment of choice is removal of pituitary gland (transsphenoidal hypophysectomy) via nasal technique. Complications include Increased ICP, bleeding, rhinorrhea, and meningitis.
- New micro-surgical techniques have been very successful in the treatment of acromegaly. Used to reduce trauma.
- If surgical risk, may undergo series of radiation treatments over 4-6 weeks and then have tumor fragments removed.
- Frequent monitoring necessary for tumor recurrence.
- Physical changes irreversible
- Removal or destruction of pituitary tissue will require replacement therapy with thyroid hormone, corticosteroids, antidiuretic hormone (ADH), and sex hormones (Timby & Smith, 2013, p. 757).
- Medication treatment includes oral treatment of bromocriptine mesylate (Parlodel), an oral antiparkinsonism inhibiting release of GH in clients with acromegaly, or cabergoline (Dostinex), or parenteral injections
Review page 758 in Timby & Smith for information on these drugs.
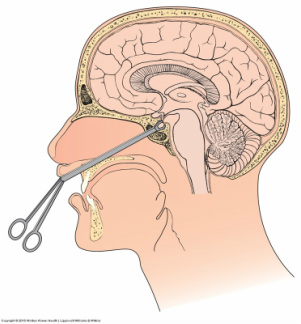
Transsphenoidal hypophysectomy- removal of pituitary gland
Source: Timby & Smith, 2013, p. 758
Lippincott Williams & Wilkins
Nursing Management
- Nursing priorities are to help the client cope with physical changes, pace
activities to prevent fatigue, relieve discomfort from headaches, abdominal
distention r/t organ enlargement, and skeletal pain. - Encourage self-care and activities when strength permits.
- Provide pharmacologic and no pharmacologic interventions for joint pain.
- Prepare for radiation therapy of pit gland, if prescribed.
- Prepare for hypophysectomy, if planned.
- Postoperatively: Monitor VS, LOC, perform frequent neuro assessments, monitor for signs of increased ICP, and meningitis.
- Elevate HOB
- Administer corticosteriods as prescribed, on time
- Monitor for adrenal insufficiency
- Monitor nasal drainage for cerebrospinal fluid (CSF).
- Monitor for F & E values
- Monitor for diabetes insipidus due to ADH disturbances
–Avoid water intoxification - Remind to avoid drinking from straws, sneezing, coughing, and bending over to prevent graft dislodgement.
Gigantism
Description
•Results from hyper secretion of GH by the anterior pituitary gland that causes hyperplasia of anterior pituitary or may be caused by defect in hypothalamus, which causes anterior pituitary to release excess amounts of GH
•Occurs in childhood before puberty – before closure of epiphyses
•There is an overgrowth of the long bones
– children may grow as tall as 8 feet and weigh over 300 pounds
•Results from hyper secretion of GH by the anterior pituitary gland that causes hyperplasia of anterior pituitary or may be caused by defect in hypothalamus, which causes anterior pituitary to release excess amounts of GH
•Occurs in childhood before puberty – before closure of epiphyses
•There is an overgrowth of the long bones
– children may grow as tall as 8 feet and weigh over 300 pounds
Data collection
•Overgrowth of long bones
•Increased height in early adulthood
•Deterioration of mental and physical status
•Labs to evaluate GH levels
Prognosis
•Lifespan is shorter than average individual
•Overgrowth of long bones
•Increased height in early adulthood
•Deterioration of mental and physical status
•Labs to evaluate GH levels
Prognosis
•Lifespan is shorter than average individual
Points to remember:
•OVERSECRETION OF GH BEFORE PUBERTY
•CHRONIC, PROGRESSIVE DISORDER, STARTLING SKELETAL GROWTH
•OVERSECRETION OF GH BEFORE PUBERTY
•CHRONIC, PROGRESSIVE DISORDER, STARTLING SKELETAL GROWTH
Simmonds' Disease (panhypopituitarism)
Pathophysiology
Rare, affects all hormones of anterior pituitary gland
Caused by destruction of pituitary followed by decreased hormone activity.
Causes:
–Postpartum emboli
–Hemorrhage
–Surgery
–Tumor
–TB
Rare, affects all hormones of anterior pituitary gland
Caused by destruction of pituitary followed by decreased hormone activity.
Causes:
–Postpartum emboli
–Hemorrhage
–Surgery
–Tumor
–TB
Assessment Findings
- Atrophied gonads and genitalia
- Impaired pituitary stimulus: thyroid and adrenals fail to secrete hormones
- hypothyroidism
- hypoglycemia
- adrenal insufficiency (Addison's Disease)
- premature aging
- extremely cachectic
- labs show decreased hormone levels (thyroid, corticosteroid, reproductive hormones)
Medical Management
Fatal if untreated
Hormone replacement therapy for:
Fatal if untreated
Hormone replacement therapy for:
- GH (bones and muscles) only for children
- ACTH (adrenals)
- TSH (thyroid)- levothyroxine (Synthroid) or liothyronine (Cytomel) for life
- FSH (reproduction)
- LH (ovulation)
- Males- testosterone
- Females- estrogen
Nursing Management
- Administer replacement hormones
- Teach medication compliance
- Monitor blood hormone levels
- Assess mental status, emotional state, energy level, and appetite
- Monitor nutrition status
- Patients tolerate 4-6 small meals per day better than 3 regular meals
Dwarfism
Dwarfism is a category of disorders with many subtypes. Its definition is vague but basically means that these children are profoundly growth-delayed for their gestational age.
Description
–hyposecretion or deficiency of GH
–occurs in childhood
•Data collection
–retarded physical growth
–premature aging
–low intellectual development
–dry skin
–sexual development delayed
Description
–hyposecretion or deficiency of GH
–occurs in childhood
•Data collection
–retarded physical growth
–premature aging
–low intellectual development
–dry skin
–sexual development delayed
Achondroplasia
The disorder causes a type of dwarfism that is recognized by its characteristic normal to large-sized head, shortened
arms and legs (especially the upper arm and thigh), a normal-sized trunk, and waddling gait. Achondroplasia is the most common type of dwarfism.
The disorder causes a type of dwarfism that is recognized by its characteristic normal to large-sized head, shortened
arms and legs (especially the upper arm and thigh), a normal-sized trunk, and waddling gait. Achondroplasia is the most common type of dwarfism.
•Implementation
–emotional support
–allow to express feelings
–prepare to administer human growth hormone
•Prognosis
–can lead normal lives
–emotional support
–allow to express feelings
–prepare to administer human growth hormone
•Prognosis
–can lead normal lives
Hypopituitarism
– Rare
•May be due to infection, autoimmune disorders, tumors, or destruction of the gland
•Failure to secrete GH is the most common abnormality
Treatment similar to Simmond's Disease
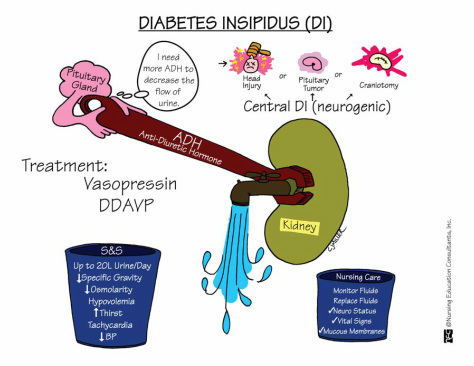
Diabetes Insipidus
What is Diabetes Insipidus?
DI is a disorder characterized by the excretion of large volumes of urine due to hyposecretion or deficiency of ADH (neurogenic DI) or failure of kidney tubular reabsorption of water (nephrogenic DI). Both have same symptoms, however in nephrogenic DI, the ADH secretion is normal; the renal tubules are the ones that fail to respond to ADH.
DI is a disorder characterized by the excretion of large volumes of urine due to hyposecretion or deficiency of ADH (neurogenic DI) or failure of kidney tubular reabsorption of water (nephrogenic DI). Both have same symptoms, however in nephrogenic DI, the ADH secretion is normal; the renal tubules are the ones that fail to respond to ADH.
- diabainein:Greek, "to pass through"
- insipidus: Latin, "having no flavor"
- Also known as "water diabetes," it is often mistaken for diabetes mellitus/sugar diabetes. It is a rare disease, not widely diagnosed, in which the kidneys produce abnormally large volumes of dilute urine.
- abnormal increase in urine output, fluid intake and often thirst.
- It causes symptoms such as urinary frequency, nocturia (frequent awakening at night to urinate) or enuresis (involuntary urination during sleep or "bedwetting").
- Urine output is increased because it is not concentrated normally.
- Consequently, instead of being a yellow color, the urine is pale, colorless or watery in appearance and the measured concentration (osmolality or specific gravity) is low
Causes
- deficient ADH
- trauma
- tumor
- surgery (i.e. hypophysectomy)
- CVA
- aneurysm
- infections
- congenital
- medications (lithium, demeclocycline, amphotericin B
Universal Symptoms of Diabetes Insipidus:
Weakness, dehydration, and weight loss develop
- Increased thirst
- Increased drinking
- Increased urination
Weakness, dehydration, and weight loss develop
Diagnostic Findings
- Fluid deprivation test (differentiates neurogenic from nephrogenic): withhold fluid for 5-6 hours. Urine volume, specific gravity, and osmalility measured at this time. After fasting phase, client is given infusion of desmopressin acetate (DDAVP), synthetic analog of vasopressin. If urine concentrates post infusion, then diagnosed with insufficient ADH (neurogenic DI). If urine still dilute with low specific gravity, then nephrogenic DI because renal tubules do not respond to ADH.
Source: NEC
Memory Notebooks
Medical Management
Be sure to ask patient what other medications they are on to ensure there is no interaction with vasopressin, examples include norepinephrine, anticoagulants, lithium, chlorpramide, etc. See Roach text p. 431 for additional list of medications and their interactions.
- Desmopressin (DDAVP) nasal solution and lypressin (Diapid) nasal spray are synthetic ADH drugs used to reduce urine output to 2-3 L/ 24 hours
- IV fluid replacement if oral intake not feasible- replaces excessive fluid volume loss
Be sure to ask patient what other medications they are on to ensure there is no interaction with vasopressin, examples include norepinephrine, anticoagulants, lithium, chlorpramide, etc. See Roach text p. 431 for additional list of medications and their interactions.
- For nephrogenic DI, restriction of Na+
- Thiazide diuretics such as hydrocholorthiazide (HydroDIURIL) will cause water loss at different site, thus lowering fluid loss than in an untreated state (Timby & Smith, p. 759).
- May combine thiazide diuretic with spironolactone or amiloride, potassium-sparing diuretics to prevent hypokalemia.
- Indomethacin (Indocin), an anti-inflammatory, may be prescribed to reduce prostaglandin E2,
- Restriction of dietary protein to reduce kidney workload in excreting protein nitrogenous wastes.
Nursing Management
Prognosis depends on etiology
- Correct fluid volume deficit- monitor IV fluid replacement
- Monitor VS, neuro, CV status
- Monitor electrolytes
- Monitor intake and output
- Daily weights
- Assess for thirst
- Change in urine appearance or volume
- Dizziness
- Weakness
- Fainting
- Palpitations
- Patient Education on maintaining hydrated and reducing fluid loss: staying indoors during hot and humid weather, avoiding strenuous physical activity.
- Stress compliance with drug therapy.
- Encourage patient to wear medic-alert bracelet
Prognosis depends on etiology
Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH)
SIADH is characterized by renal reabsorption of water than its normal excretion.
Disorder of posterior pituitary gland in which an increased or a continued release of the ADH occur in response to ADH, kidneys reabsorb more water, resulting in water intoxication-characterized by fluid retention, hyponatremia, hemodilution, and fluid overload without peripheral edema, concentrated urine – decreased
urine output
Increased ADH leads to increased water retention [excess ADH increases renal tubular permeability and reabsorption of water into the circulation. Consequently, extracellular fluid volume expands, plasma osmolality declines, the glomerular filtration rate rises, and sodium levels decline.
CAUSES:
Disorder of posterior pituitary gland in which an increased or a continued release of the ADH occur in response to ADH, kidneys reabsorb more water, resulting in water intoxication-characterized by fluid retention, hyponatremia, hemodilution, and fluid overload without peripheral edema, concentrated urine – decreased
urine output
Increased ADH leads to increased water retention [excess ADH increases renal tubular permeability and reabsorption of water into the circulation. Consequently, extracellular fluid volume expands, plasma osmolality declines, the glomerular filtration rate rises, and sodium levels decline.
CAUSES:
- CNS disorders
- CVA
- Head trauma
- Lung tumors
- Brain tumors, trauma or
infection - Drugs – including vasopressin, general anesthetic agents,
oral hypoglycemics, and triclic antidepressants
- More prevalent in older adult clients
Assessment
- Main symptoms initially reflect effects of hyponatremia and water retention
- As condition becomes more severe, HA, weakness, muscle cramps or twitching, anorexia, nausea and vomiting, irritability and weight gain without edema
- When CNS is affected by water intoxication, LOC deteriorates, - seizures and coma may result
- Decreased serum sodium levels and osmolarity
- Urine sodium and osmolarity high
Medical Management
- Treatment aimed at eliminating underlying cause
- Correct water retention
with osmotic diuretics such as mannitol and loop diuretics such as
furosemide - Treat severe hyponatremia with IV 3% hypertonic NaCl
solution.
Nursing Management
- Monitor fluid intake and output and VS
- Assess LOC and report changes to physician
- Monitor for signs of fluid overload (confusion, dyspnea, pulmonary congestion, hypertension) and hyponatremia (weakness, muscle cramps, anorexia, nausea, diarrhea, irritability, headache, weight gain without edema)
- Client/Family Education regarding medication schedule and SE of therapy.
- Stress medication compliance and staying on schedule
