Hyperparathyroidism
Description
A condition involving increased secretion of parathyroid hormone PTH. Can be a primary or secondary condition.
When the parathyroid malfunctions, calcium and phosphorus levels are affected, resulting in increased urine excretion of phosphorus and loss of calcium from bones. Bones become demineralized as calcium leaves and enters bloodstream. Renal stones may develop as calcium becomes concentrated in urine.
Primary hyperparathyroidism is caused by adenoma of one of the parathyroid glands.
Secondary hyperparathyroidism, parathyroid secretes PTH in response to low calcium in blood stream, resulting from Vitamin D deficiency, chronic renal failure, large doses of thiazide diuretics, as well as excessive laxative and calcium use (Timby & Smith, 2013, p.771).
A condition involving increased secretion of parathyroid hormone PTH. Can be a primary or secondary condition.
When the parathyroid malfunctions, calcium and phosphorus levels are affected, resulting in increased urine excretion of phosphorus and loss of calcium from bones. Bones become demineralized as calcium leaves and enters bloodstream. Renal stones may develop as calcium becomes concentrated in urine.
Primary hyperparathyroidism is caused by adenoma of one of the parathyroid glands.
Secondary hyperparathyroidism, parathyroid secretes PTH in response to low calcium in blood stream, resulting from Vitamin D deficiency, chronic renal failure, large doses of thiazide diuretics, as well as excessive laxative and calcium use (Timby & Smith, 2013, p.771).
Assessment
S & S
Diagnostic Findings
Diagnosis is based on laboratory findings:
S & S
- Depressed response of peripheral nerves due to excessive calcium
- Fatigue and muscular weakness
- Loss/decrease of muscle tone
- Cardiac dysrhythmias may develop due to the high calcium (recall calcium's role in muscular activity, especially the heart)
- Skeletal tenderness and pain with weight bearing (due to calcium loss in bones)
- Osteoporosis- leads to brittle bones breaking with little to no trauma (pathologic fractures)
- Nausea
- Vomiting
- Constipation
- Large amounts of calcium and phosphorus passing through kidney may cause kidney stones in urinary tract, pyelonephritis, and uremia
Diagnostic Findings
Diagnosis is based on laboratory findings:
- Serum calcium which will be elevated and the phosphorus level will be decreased without other causes of hypercalcemia.
- 24 hour urine test shows increased calcium levels in the urine
- Skeletal x-rays show loss of calcium in the bones
- MRI or CT help to identify parathyroid adenoma (if present)
- PTH levels are elevated
Medical and Surgical Management
Treating the underlying cause is the path to treatment.
Treating the underlying cause is the path to treatment.
- Secondary hyperparathyroidism will be managed by correcting the cause (Vitamin D therapy for deficiency, correct renal failure, restrict calcium in diet).
- Sodium and phosphorus electrolytes are replaced.
- Warning: Hormone replacement with synthetic calcitonin (Calcimar) may cause allergic reaction and drug resistance. Drug resistance may cause antibodies to neutralize the hormone.
- Primary hyperparathyroidism treatment is more aggressive. Surgical removal of the enlarged glandular tissue or tumor of one of the parathyroid glands is performed.
- The physician will determine how many parathyroid glands (recall there are 4 usually) to remove, based on the cause and laboratory/diagnostic results.
- One or more of the glands are left for calcium and phosphorus metabolism.
Nursing Management
The primary nursing responsibility is to teach the patient about the disease process and the toll the disease can take on their health if not managed correctly, as well as the planned medical management and importance of following the prescribed treatment.
Other nursing interventions include:
The primary nursing responsibility is to teach the patient about the disease process and the toll the disease can take on their health if not managed correctly, as well as the planned medical management and importance of following the prescribed treatment.
Other nursing interventions include:
- Careful measurement of I & Os
- Straining urine for calculi (kidney stones)
- Observe for signs of urinary calculi: flank pain and decreasing urinary output
- Increase fluid intake to keep urine diluted (at least 3-4 Liters of fluid daily)
- Encourage low calcium diet (fewer dairy products)
- Assess ability for self-care
- Provide a safe environment (prevent falls and injury)
- Provide frequent rest periods due to the fatigue
- Assess fatigue level frequently
Hypoparathyroidism
Hypoparathyroidism results from an inadequate amount of circulating PTH; it is not a common endocrine problem.
It results in hypocalcemia due to lack of PTH production to maintain serum calcium levels. Recall that PTH regulates calcium balance by increasing absorption of calcium from GI tract and bone resorption of calcium. Hypocalcemia affects neuromuscular functions. It causes hyperexcitability, resulting in spastic muscle contractions and paresthesias (abnormal sensations).
Etiology: The most common cause is accidental removal of or damage to the vascular supply of the glands during neck surgery
(thyroidectomy, radical neck surgery).
Idiopathic causes would due to an autoimmune response or congenital absence of the parathyroid glands. This however, is not very common.
(Timby & Smith, 2013, p. 772)
It results in hypocalcemia due to lack of PTH production to maintain serum calcium levels. Recall that PTH regulates calcium balance by increasing absorption of calcium from GI tract and bone resorption of calcium. Hypocalcemia affects neuromuscular functions. It causes hyperexcitability, resulting in spastic muscle contractions and paresthesias (abnormal sensations).
Etiology: The most common cause is accidental removal of or damage to the vascular supply of the glands during neck surgery
(thyroidectomy, radical neck surgery).
Idiopathic causes would due to an autoimmune response or congenital absence of the parathyroid glands. This however, is not very common.
(Timby & Smith, 2013, p. 772)
Assessment
Tetany is the main symptom of acute and sudden hypoparathyroidism.
Abnormal labs include decreased serum calcium and PTH levels and increased serum phosphate levels – in urine, both levels are decreased.
Tetany is the main symptom of acute and sudden hypoparathyroidism.
- This state is characterized by tingling of lips, hands, fingers, and occasionally feet, leading to increased muscle tension, paresthesias, and stiffness.
- Dysphagia, painful tonic spasms of smooth and skeletal musculature, a constricted feeling in throat, and laryngospasms are also present.
- Chvostek’s sign (facial muscle spasm when face is tapped below temple). Causes twitching of mouth, nose, and eye, jaw tightens (see video below for real patient with positive Chvostek's sign).
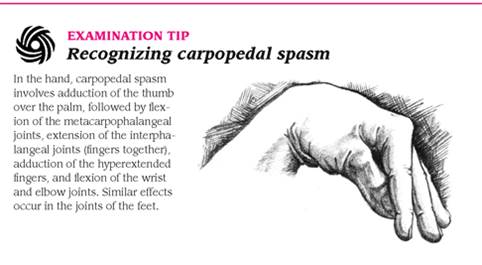
- Trousseau’s sign (carpopedal spasm – hand flexes inward when arterial circulation is interrupted by applying
a blood pressure cuff for 3 minutes) are positive. See video below to get a real-life look at Trousseau's sign. - Respiratory function may be severely compromised by muscle spasm and airway obstruction due to laryngospasms.
- Cyanosis may be present from airway constriction
- Asphyxia and cardiac dysrhythmias may occur from respiratory complications
- Client may experience nausea, vomiting, abdominal pain, seizures…are usually anxious and apprehensive.
- In chronic hypoparathyroidism, neuromuscular irritability may occur along with constipation or diarrhea, numbness and tingling of arms and legs, loss of tooth enamel, and muscular pain. "Positive Chvostek's sign and Trousseau's sign may or may not be elicited, depending on the degree of hypocalcemia" (Timby & Smith, 2013, p. 772).
Abnormal labs include decreased serum calcium and PTH levels and increased serum phosphate levels – in urine, both levels are decreased.

Source: Unknown
|

Source: unknown
|
Source: unknown
|
Medical Management
- IV calcium salt (calcium gluconate) is used to treat tetany and severe hypoparathyroidism.
- May require ET intubation and mechanical ventilation for acute respiratory distress
- Bronchodilators administered
- Parathyroid replacement (calcitonin) not usually done due to incidence of allergic reactions
- Long-term treatment includes:
- Oral calcium replacement along with Vitamin D replacement or Vitamin D2 (calciferol) to increase calcium level
- Dose is given according to severity of hypocalcemia
- Frequent monitoring of serum and urine calcium levels
- Oral phosphate binders (Amphogel) to decrease phosphate levels
- Diet high in calcium and low in phosphorus is recommended
Nursing Management
Be alert for S & S of tetany
Be alert for S & S of tetany
- Assess for Chvostek's and Trousseau's signs
- Monitor client for increasing severity of symptoms (w/chronic hypoparathyroidism)
- Administer IV calcium salt if needed and observe for adverse effects (flushing, cardiac dysrhythmia- usually bradycardia, tingling in arms and legs, and metallic taste in mouth.
- Monitor for local tissue necrosis if IV infiltrates.
- Monitor serum Ca+ levels to ensure treatment is working
- For chronic hypoparathyroidism, obtain complete history- medical, drug, and allergy
- Examine for symptoms of disorder: arms and legs for spasms, ausculate lungs for dyspnea, vital signs for cardiac dysrhythmias. Pay attention to heart rate and rhythm.
- Maintain emergency trach tray avilable, mechanical ventilation equipment, artificial airway, ET intubation equipment at bedside.
- Observe for respiratory distress or dyspnea- notify MD ASAP
- Assist client with ADLs
- Keep environment quiet and reduce stimulating disturbances which can trigger contractions or convulsions
- Patient education if treatment is life-long--- diet, medication compliance, medication SE, and adverse rxns
- Education on diet: may need consultation with dietician; read food labels carefully, avoid carbonated drinks as they contain high phosphorus levels as phosphoric acid, encourage increased intake of calcium-rich foods such as milk, yogurt, green leafy vegetables, and fortified orange juice
Additional Resources:
Hypoparathyroidism Answers: http://hypoparathyroidism.com/what-is-hypoparathyroidism/
Mayo Clinic Hypoparathyroidism: http://www.mayoclinic.com/health/hypoparathyroidism/DS00952/DSECTION=treatments-and-drugs
Hypopara.org: https://www.hypopara.org/wwwroot/userfiles/files/a_guide_to_hypoparathyroidism.pdf
Hypoparathyroidism Answers: http://hypoparathyroidism.com/what-is-hypoparathyroidism/
Mayo Clinic Hypoparathyroidism: http://www.mayoclinic.com/health/hypoparathyroidism/DS00952/DSECTION=treatments-and-drugs
Hypopara.org: https://www.hypopara.org/wwwroot/userfiles/files/a_guide_to_hypoparathyroidism.pdf
