It is important to understand that thyroid disorders can often times be difficult to recognize because the symptoms are vague and mimic many other disorders. It is not until the disease advances to severe level that it is diagnosed and treated. Treatment for thyroid disorders is a long-term ordeal so it is important when providing education on the disorder that patients understand the importance of periodic follow up and compliance with treatments.
Hyperthyroidism
 Timby & Smith, 2013, p. 760
Lippincott Williams & Wilkins
Timby & Smith, 2013, p. 760
Lippincott Williams & Wilkins
Hyperthyroidism is when there is an overproduction of thyroid hormones from the thyroid. It has also been called Grave's Disease, Basedow's disease, thyrotoxicosis, and exophthalmic goiter.
Hyperthyroidism is not caused by only one factor. It is believed that perhaps it is autoimmune or inherited. The over-secretion of thyroid hormones follows ailments such as thyroid tumors, pituitary tumors, and hypothalamic malignancies (Timby & Smith, 2013). It is also thought to result from stress or infections, which put stress on the body's normal physiologic processes. As a result of the overproduction of T3 and T4, the thyroid hormones, the metabolic rate will increase. Recall that the thyroid's hormones are responsible for regulating metabolic rate. When the hormone levels are high, the metabolic rate will increase. When the hormone levels are low, the rate will decrease as is the case in hypothyroidism which is discussed later in this section. Women are more likely to have hyperthyroidism. In fact, the incidence
is 6 X’s greater in women than in men, and
highest frequency is in the 30 to 50 year old age group.
•Affects all major organ systems of body
•Iodine deficiency is believed to predispose clients to this and other thyroid diseases
•Most common form of hyperthyroidism is Grave’s disease
•Followed by multinodular goiter, more common in older women.
•Affects all major organ systems of body
•Iodine deficiency is believed to predispose clients to this and other thyroid diseases
•Most common form of hyperthyroidism is Grave’s disease
•Followed by multinodular goiter, more common in older women.
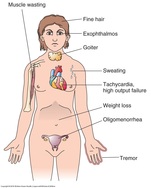
Assessment Findings
Signs and symptoms vary from mild to severe.
Typical symptoms are:
Review Table 50-1 on page 761 in Timby & Smith, 2013 to compare the signs and symptoms of hyperthyroidism and hypothyroidism related to the various body systems.
Signs and symptoms vary from mild to severe.
Typical symptoms are:
- restlessness, yet feeling fatigued and weak
- highly excitable
- tachycardia which can result in heart failure
- constantly agitated
- fine tremors of hands, clumsiness
- heat intolerance
- increased appetite, weight loss
- diarrhea
- visual changes: blurry or double vision
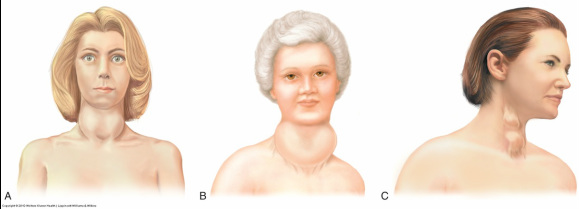
- EXOPHTHALMOS seen in severe hyperthyroidism, where eyes protrude from orbit (r/t muscle and fatty tissue accumulation on lateral and posterior eyeball (see image below).
- Neck swelling caused by enlarged gland (goiter)
Review Table 50-1 on page 761 in Timby & Smith, 2013 to compare the signs and symptoms of hyperthyroidism and hypothyroidism related to the various body systems.
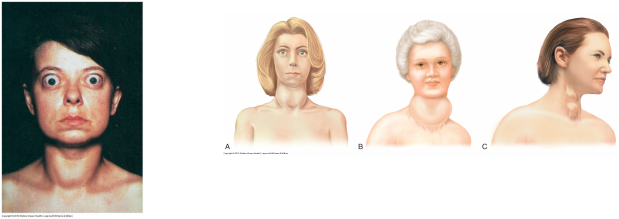
Image A: Exophthalmos figure 49-9
Image B: Goiter
Source: Timby & Smith, 2013
Lippincott Williams and Wilkins
Diagnostic Findings
Serum blood tests are performed and show that protein bound iodine, free thyroxine (FT4), thyroglobulin, and serum T3 and T4 levels are elevated. The TSH level is decreased as a result of the elevated thyroid hormones.
Serum blood tests are performed and show that protein bound iodine, free thyroxine (FT4), thyroglobulin, and serum T3 and T4 levels are elevated. The TSH level is decreased as a result of the elevated thyroid hormones.
- Thyroid ultrasound shows an enlarged thyroid gland.
- Thyroid scan shows an increased uptake of radioactive iodine (RAI, 131 I and 123 I) throughout the gland or is confined to a single nodule (Timby & Smith, p. 763).
- The iodine isotope used for diagnostics does not destroy the thyroid gland.
Medical Management
Management of hyperthyroidism is handled by prescribing antithyroid medications such as propylthiouracil (PTU, PropylThyracil) and methimazole (Tapazole), used to block production of thyroid hormone prior to surgery or as long term treatment for those clients who are not surgical candidates or for radiation treatment (p. 761).
•Propylthiouracil inhibits TH production, decreases vascularity and returns gland to euthyroid state
•Iodine given in large doses blocks synthesis and release of TH, decreases size and vascularity of thyroid, making resection easier and safer. It is a common method for surgical preparation. Generalized system reactions to these drugs include: hay fever, sore throat, skin rash, fever, headache, nausea, vomiting, paresthesias. Severe systemic reactions include: agranulocytosis (decrease in WBCs) and granulocytopenia, hypothrombinemia, and exfoliative dermatitis (Roach & Ford, 2010, p. 450).
--Iodine therapy with administration of propylthiouracil for 7-10 days before surgery is common method for surgical preparation of client with hyperthyroidism.
As with all medication compliance education it is important to inform clients that non compliance with "prescription therapy early in its management, the disorder may reactivate" (p. 761). According to Timby and Smith (2013), approximately 40-70% of those compliant with antithyroid medication therapy for 1-2 years have achieved remission. Follow up care is essential to detecting any signs of recurrence.
Potassium iodide (Lugol's solution) may also be prescribed along with an antithyroid drug.
Potassium iodide "creates a negative feedback effect on the hypothalamus" so then hypothalamus will sense a rise of iodine levels, therefore suppressing secretion of thyroid-releasing hormone and consequently thyroid hormone levels are reduced (p. 761).
Using potassium iodide and an antithyroid drug can curtail thyroid activity prior to surgery and reduces post-op complications of bleeding and thyrotoxicosis.
It is important to note that antithyroid drugs are avoided during pregnancy to reduce the risk of the fetus developing cretinism (hypothyroidism of infant).
131 I is utilized to destroy the hyperplastic thyroid tissue by means of radiation which damages or destroys thyroid cells therefore causing cells to produce less TH. May require several treatments. About 6-8 weeks after initial dose, clients report improvement in their symptoms. Disadvantage is that it is difficult to determine how much thyroid tissue is being radiated so complication of hypothyroidism is not seen until long after 131 I treatment is completed. May cause dryness/irritation to mouth/throat.
Refer to Drug Therapy Table 50-1 for chart of medications used to treat thyroid disorders (p. 762)
Other Medications utilized are propranolol (Inderal) which is the most frequently used beta blocker to block effects of thyroid hormones on cardiovascular system (ex. tachycardia). These symptoms include heat intolerance, palpitations, nervousness, tremor, and muscle weakness. Propranolol is used in conjunction with other antithyroid treatment and relieves symptoms that cause discomfort in the client with hyperthyroidism.
Surgical Management
Subtotal thyroidectomy (partial removal of the thyroid gland) or partial thyroid lobectomy (removal of the upper or lower portion of one lobe) is used effectively as treatment for a confined area of nodule located within the thyroid that is increasing production of hormones (Timby & Smith, 2013, p. 763).Sometimes an entire lobe with or without the isthmus is removed.
A total thyroidectomy (entire thyroid gland is removed) can also be performed when a malignant tumor or if hyperthyroidism is too advanced and involves all the glandular tissue. Prior to surgical removal of any part of the thyroid, clients are given antithyroid drugs to help reduce the amount of hormones that the thyroid releases the blood stream during excision.
Minimally invasive endoscopic techniques are utilized for the single nodules less than 3 cm which only requires 3-4 small incisions in the neck rather than the long typical incision across the neck (see picture below).
Management of hyperthyroidism is handled by prescribing antithyroid medications such as propylthiouracil (PTU, PropylThyracil) and methimazole (Tapazole), used to block production of thyroid hormone prior to surgery or as long term treatment for those clients who are not surgical candidates or for radiation treatment (p. 761).
•Propylthiouracil inhibits TH production, decreases vascularity and returns gland to euthyroid state
•Iodine given in large doses blocks synthesis and release of TH, decreases size and vascularity of thyroid, making resection easier and safer. It is a common method for surgical preparation. Generalized system reactions to these drugs include: hay fever, sore throat, skin rash, fever, headache, nausea, vomiting, paresthesias. Severe systemic reactions include: agranulocytosis (decrease in WBCs) and granulocytopenia, hypothrombinemia, and exfoliative dermatitis (Roach & Ford, 2010, p. 450).
--Iodine therapy with administration of propylthiouracil for 7-10 days before surgery is common method for surgical preparation of client with hyperthyroidism.
As with all medication compliance education it is important to inform clients that non compliance with "prescription therapy early in its management, the disorder may reactivate" (p. 761). According to Timby and Smith (2013), approximately 40-70% of those compliant with antithyroid medication therapy for 1-2 years have achieved remission. Follow up care is essential to detecting any signs of recurrence.
Potassium iodide (Lugol's solution) may also be prescribed along with an antithyroid drug.
Potassium iodide "creates a negative feedback effect on the hypothalamus" so then hypothalamus will sense a rise of iodine levels, therefore suppressing secretion of thyroid-releasing hormone and consequently thyroid hormone levels are reduced (p. 761).
Using potassium iodide and an antithyroid drug can curtail thyroid activity prior to surgery and reduces post-op complications of bleeding and thyrotoxicosis.
It is important to note that antithyroid drugs are avoided during pregnancy to reduce the risk of the fetus developing cretinism (hypothyroidism of infant).
131 I is utilized to destroy the hyperplastic thyroid tissue by means of radiation which damages or destroys thyroid cells therefore causing cells to produce less TH. May require several treatments. About 6-8 weeks after initial dose, clients report improvement in their symptoms. Disadvantage is that it is difficult to determine how much thyroid tissue is being radiated so complication of hypothyroidism is not seen until long after 131 I treatment is completed. May cause dryness/irritation to mouth/throat.
Refer to Drug Therapy Table 50-1 for chart of medications used to treat thyroid disorders (p. 762)
Other Medications utilized are propranolol (Inderal) which is the most frequently used beta blocker to block effects of thyroid hormones on cardiovascular system (ex. tachycardia). These symptoms include heat intolerance, palpitations, nervousness, tremor, and muscle weakness. Propranolol is used in conjunction with other antithyroid treatment and relieves symptoms that cause discomfort in the client with hyperthyroidism.
Surgical Management
Subtotal thyroidectomy (partial removal of the thyroid gland) or partial thyroid lobectomy (removal of the upper or lower portion of one lobe) is used effectively as treatment for a confined area of nodule located within the thyroid that is increasing production of hormones (Timby & Smith, 2013, p. 763).Sometimes an entire lobe with or without the isthmus is removed.
A total thyroidectomy (entire thyroid gland is removed) can also be performed when a malignant tumor or if hyperthyroidism is too advanced and involves all the glandular tissue. Prior to surgical removal of any part of the thyroid, clients are given antithyroid drugs to help reduce the amount of hormones that the thyroid releases the blood stream during excision.
Minimally invasive endoscopic techniques are utilized for the single nodules less than 3 cm which only requires 3-4 small incisions in the neck rather than the long typical incision across the neck (see picture below).

Note the long incision across the neck.
Source: Unknown
- Surgical Complications of thyroidectomy include the following:
- *Accidental removal or alteration in the blood supply to the parathyroid glands(which are embedded in thyroid tissue), resulting in hypocalcemia. Can be transplanted to nearby muscular tissue and function can be restored.
- *Hemorrhage due to the vascularity of the thyroid and surrounding tissue
- *Thyrotoxicosis (thyroid storm) resulting from excessive thyroid hormone released during surgical incision
- *Damage to the recurrent laryngeal nerve, which affects vocal cord function. Damage of this nerve leads to impaired breathing due to vocal cords unable to open properly during inspiration, the voice may sound weak, hoarse or breathy; aspiration and pneumonia may occur if vocal cords do not close completely during swallowing.
Nursing Management
•Signs and symptoms of hyperthyroidism are alleviated as much as possible and cardiac problems must be controlled before surgery
•If iodine is used, pt must be assessed for signs of iodine toxicity such as swelling of buccal mucosa and other mucous membranes, excessive salivation, nausea and vomiting, and skin reactions
•If these reactions occur, iodine administration should be discontinued and MD notified
•Iodine should be mixed with water or juice, sipped through a straw, and administered after meals
•Preop teaching – cough, deep breathing, and leg exercise taught and practiced
•Teach how to support head manually while turning in bed, this will decrease stress on suture line after surgery.
•ROM exercises of neck should be practiced
•Explain routine postop care
Post-op care -
•Risks:
– hemorrhage, AW obstruction, paralysis of laryngeal nerve, hypoparathyroidism, hypothyroidism
See Nursing Care Plan 50-1 p. 764-766 for more care of the client undergoing thyroid surgery.
(Timby & Smith, 2013, p. 763)
- Monitor heart rate and BP
- Record sleep pattern and daily weights
- Promote rest and help client avoid excess physical stimulation
- Teach regarding increased caloric intake to meet increased metabolic needs, about 6 full meals a day + snacks
- –high protein, carbs,minerals, vitamins esp.B-complex and ascorbic acid (for collagen synthesis); Avoid highly seasoned foods, Avoid coffee, tea, cola (due to caffeine content); Encourage milk; Dietitian consult
- Educate about antithyroid therapy effects taking several weeks to be apparent
- Address concerns over RAI affecting other tissues besides thyroid tissue. Only affects thyroid tissue.
- Warn about possible transient effects after treatment with 131 I and 123 I: nausea, vomiting, malaise, fever, and gland tenderness.
- Teach and demonstrate to patient to support the neck with the hands when rising to sit (see image below) to prevent strain to the neck muscles and surgical incision (p.767).
- Sit patient in a high-fowlers position in order to promote drainage and to prevent from straining neck when lifting head.
•Signs and symptoms of hyperthyroidism are alleviated as much as possible and cardiac problems must be controlled before surgery
•If iodine is used, pt must be assessed for signs of iodine toxicity such as swelling of buccal mucosa and other mucous membranes, excessive salivation, nausea and vomiting, and skin reactions
•If these reactions occur, iodine administration should be discontinued and MD notified
•Iodine should be mixed with water or juice, sipped through a straw, and administered after meals
•Preop teaching – cough, deep breathing, and leg exercise taught and practiced
•Teach how to support head manually while turning in bed, this will decrease stress on suture line after surgery.
•ROM exercises of neck should be practiced
•Explain routine postop care
Post-op care -
•Risks:
– hemorrhage, AW obstruction, paralysis of laryngeal nerve, hypoparathyroidism, hypothyroidism
See Nursing Care Plan 50-1 p. 764-766 for more care of the client undergoing thyroid surgery.
(Timby & Smith, 2013, p. 763)

Figure 50-5 Timby & Smith, 2013, p. 767
Lippincott Williams & Wilkins
Grave's Disease
Note that Grave's Disease is similar to hyperthyroidism although it is generally classified as a multi-system autoimmune syndrome.
Cause:
Many factors: autoimmune reactions, excess secretion of TSH by pituitary gland, thyroiditis, neoplasms, excessive intake of thyroid meds.
•Generally classified as a multi-system autoimmune syndrome marked by increased production of thyroid hormone…secretion of excessive amounts of thyroid hormone in blood causes and increase in metabolic processes
•More frequent in women under age 40
•Characterized by remissions and exacerbations, with or without treatment.
•May progress to destruction of thyroid tissue, causing hypothyroidism
Precipitating factors:
--Insufficient iodine supply, infections, and emotions may interact with genetic factors that
control immune and metabolic activities
Data collection
•Diffuse enlargement of thyroid gland
•Expothalamos in severe hyperthyroidism
•Fatigue, difficulty sleeping, hand tremors, changes in menstruation ranging from decreased flow to amenorrhea
•Older clients may present wit atrial fibrillation, angina, or CHF
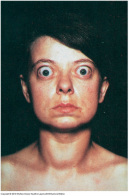
Exophthalmos
(forward protrusion of eyeballs due to accumulation of fat deposits and inflammation in retro-orbital (rear and sides of eyeball)
Eye Care for exophthalmos
Eye care: if exophthalmos is present, potential for corneal injury due to dryness and irritation. May have orbital pain.
Cause:
Many factors: autoimmune reactions, excess secretion of TSH by pituitary gland, thyroiditis, neoplasms, excessive intake of thyroid meds.
•Generally classified as a multi-system autoimmune syndrome marked by increased production of thyroid hormone…secretion of excessive amounts of thyroid hormone in blood causes and increase in metabolic processes
•More frequent in women under age 40
•Characterized by remissions and exacerbations, with or without treatment.
•May progress to destruction of thyroid tissue, causing hypothyroidism
Precipitating factors:
--Insufficient iodine supply, infections, and emotions may interact with genetic factors that
control immune and metabolic activities
Data collection
•Diffuse enlargement of thyroid gland
•Expothalamos in severe hyperthyroidism
•Fatigue, difficulty sleeping, hand tremors, changes in menstruation ranging from decreased flow to amenorrhea
•Older clients may present wit atrial fibrillation, angina, or CHF
Exophthalmos
(forward protrusion of eyeballs due to accumulation of fat deposits and inflammation in retro-orbital (rear and sides of eyeball)
- seen in 20-40 % of patients with Grave's disease
- Sclera is often visible above iris
- upper lids retracted
- person has characteristic unblinking stare
- Usually bilateral, but may involve only one eye
- may experience blurred vision, eye pain, lacrimation, and photophobia
- inability to close eyelid over protruding eyeballs increases risk of corneal dryness, irritation, infection, and ulceration
Eye Care for exophthalmos
Eye care: if exophthalmos is present, potential for corneal injury due to dryness and irritation. May have orbital pain.
- To relieve eye discomfort, application of liquid tears to soothe and
moisten conjunctival membranes. - Salt restriction may help to reduce periorbital edema,
- Elevation of client’s head promotes fluid drainage (pt should sit upright as much as possible).
- Dark glasses to reduce glare and prevent irritation from dust and dirt.
- Poss. tape eyelids closed for sleep, if can’t close.
- Good grooming can be helpful in reducing loss of self-esteem that results from altered body image. May need surgery if severe exophthalmos.
Goiter
Euthyroid (normal thyroid state)
Euthyroid goiter (enlargement of a normal thyroid gland)
Euthyroid (normal thyroid state)
Euthyroid goiter (enlargement of a normal thyroid gland)
- Enlargement of thyroid gland not caused by inflammation or neoplasm
- Three types of goiter –diffuse toxic goiter
***as found in hyperthyroidism; frequently associated with exopthalamos
–simple nontoxic goiter (endemic)
***due to iodine deficiency in diet
*******Goitrogens-- (foods, drugs) that cause goiter (cabbage, soybeans, rutabagas, peanuts, peaches, peas, strawberries, spinach, radishes…contain agents that decrease thyroxine production)
***inability of thyroid gland to use iodine
***increasing demand on thyroid hormones
–nodular goiter
***similar to simple goiter, except multiple nodules causing enlargement
*******multinodular goiter -secretes TH
Toxic multinodular goiter
•characterized by small, discrete, independently functioning nodules (palpable deformities) in
the thyroid gland tissue that secrete TH
•May be benign or malignant
•If TH levels are elevated, manifestations of hyperthyroidism occur – lower to develop and differ somewhat from Grave’s disease
•Client with this type of hyperthyroidism is usually a woman in her 60’s or 70’s who has had a goiter for a number of years
Treatment
•Drug therapy – hormone replacement with Synthroid (T4), desiccated thyroid, or liathyronine (T3)
•small doses of iodine (Lugol’s or potassium iodine solution) for goiter resulting from iodine deficiency
•avoid goitrogenic foods (soybeans, peanuts, drugs lithium)
•surgery

Photo of Goiter
Image Source: Unknown
Thyrotoxic Crisis (aka Thyroid Crisis or Thyroid Storm)
Thyrotoxic crisis is an abrupt and potentially fatal type of hyperthyroidism. It is thought to be triggered by a number of things, such as extreme stress, infection, diabetic ketoacidosis, trauma, toxemia of pregnancy, manipulation of hyperactive thyroid during surgery or physical examination (which is why meds are given prior to surgery and care is taken during examination). Although rare, this condition may occur in clients who are undiagnosed or inadequately treated hyperthyroidism (Timby & Smith, 2013, p. 763). There is an oversecretion of T3 and T4 which is followed by release of epinephrine. Metabolism increases, which is seen as a stress by the body. As a result, "the adrenal glands produce excess corticosteroids to respond to the "stress" created by the this hypermetabolic state" (p. 763).
Assessment
- high temperatures (up to 106 F or 41 C)
- rapid pulse and HR
- cardiac dysrrhythmias common
- persistent vomiting
- extreme restlessness with delirium
- chest pain
- dyspnea
Medical Management
This conditions warrants immediate treatment!
This conditions warrants immediate treatment!
- Antithyroid drugs are used to block hormone production
- IV corticosteroids administered to replace those produced by adrenals in overstimulation
- IV sodium iodide to prevent thyroid gland from releasing hormones
- Propanolol reduces tachycardia and prevents dysrrhythmias
- IV fluids, antipyretics, and oxygen therapy
Nursing Management
Requires constant assessment
Requires constant assessment
- Vital signs, especially temperature (fever from hypermetabolic state)
- Antipyretics, cooling blanket, ice application and cool room to reduce body temperature
- Implement any therapeutic measures necessary to correct.
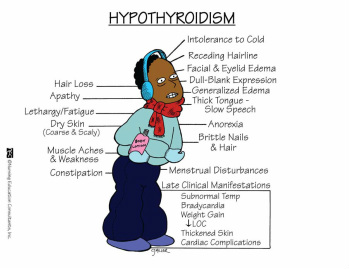
Hypothyroidism
What is HYPOTHYROIDISM ?
– The thyroid gland fails to secrete adequate amount of thyroid hormone, so thyroid hormone levels are low
Causes:
Primary hypothyroidism•Thyroid gland not producing enough TH, even though there is enough TSH, so pituitary is functioning adequately.
•The pituitary responds to low TH by producing more TSH.
–Primary cause
•Congenital defect, inflammation of thyroid gland, iodine deficiency, thyroidectomy
–TH decreased
–TSH increased
Secondary hypothyroidism (pituitary cause):
•caused by low levels of TSH (via pituitary) or thyrotropin -releasing hormone from hypothalamus, which fail to stimulate release of TH.
–TH decreased
–TSH decreased
•Most cases of hypothyroidism are primary causes.
Secondary causes due to Pituitary or hypothalamic lesion, postpartum pituitary necrosis
– The thyroid gland fails to secrete adequate amount of thyroid hormone, so thyroid hormone levels are low
Causes:
- Usually results from insufficient circulating thyroid hormone as result of a
variety of abnormalities - Autoimmune thyroiditis, surgical removal of
thyroid gland, radioactive iodine thyroid gland ablation, external irradiation,
thyroid gland/iodine defect
Primary hypothyroidism•Thyroid gland not producing enough TH, even though there is enough TSH, so pituitary is functioning adequately.
•The pituitary responds to low TH by producing more TSH.
–Primary cause
•Congenital defect, inflammation of thyroid gland, iodine deficiency, thyroidectomy
–TH decreased
–TSH increased
Secondary hypothyroidism (pituitary cause):
•caused by low levels of TSH (via pituitary) or thyrotropin -releasing hormone from hypothalamus, which fail to stimulate release of TH.
–TH decreased
–TSH decreased
•Most cases of hypothyroidism are primary causes.
Secondary causes due to Pituitary or hypothalamic lesion, postpartum pituitary necrosis
- Usually insufficient thyroid hormones
- When it occurs in infancy = cretinism
- When it occurs in childhood = juvenile hypothyroidism
- When it occurs in adulthood = myxedema (severe hypothyroidism), discussed later in this section
Assessment Findings
Can go untreated for a long period of time, years.
May be difficult to detect in older adults since many of the symptoms are similar to those of normal aging.
- Metabolic rate and physical and mental activity are slowed,
- Forgetful
- Fatigue
- Lethargic, decreased energy, dozes off frequently
- Chronic HA’s
- Bradycardia
- Wt increases despite low calorie intake
- Face is mask-like expression
- Often irritable
- Tongue may be enlarged, lips swollen, possible eyelid edema
- Temperature and pulse decreased, intolerance to cold
- Skin/hair = coarse, sparse, and falls out
- Menstrual disorders
- Constipation
- Voice low pitched, hoarse, speech slow
- Numbness or tingling in arms and legs
- May lead to enlarged heart caused by pericardial effusion and increased tendency for atherosclerosis and excessive effort by the heart to pump blood (Timby & Smith, 2013, p. 767).
- Anemia may be present also
- Difficult to recognize early symptoms since symptoms are vague and non-specific
Can go untreated for a long period of time, years.
May be difficult to detect in older adults since many of the symptoms are similar to those of normal aging.
Source: NEC 2013
Memory Notebook
Diagnostic Findings
In Primary hypothyroidism, TSH levels are elevated R/T negative feedback to pituitary gland= low levels of thyroid hormones cause pituitary gland to increase secretion of TSH.
In Primary hypothyroidism, TSH levels are elevated R/T negative feedback to pituitary gland= low levels of thyroid hormones cause pituitary gland to increase secretion of TSH.
Medical Management
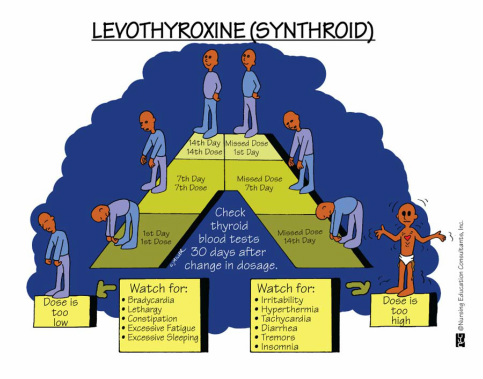
Thyroid replacement therapy such as levothyroxine (Synthroid) or liothyronine sodium (Cytomel) are oral drugs. Low dose is started and then increased or decreased until therapeutic level is reached. See Drug Therapy Table 50-1 in Timby & Smith page 762 for additional drugs used. Drugs may be required for lifetime depending on underlying cause.
The drug of choice to treat hypothyroidism is levothyroxine (Synthroid) because it is relatively inexpensive, dosed at once a day, has more uniform potency than others. For this reason it is important to educate patients not to switch to another brand(generic) unless physican has reviewed. Not all thyroid hormone replacement drugs are equivalent. It is also important to take levothyroxine in the morning on an empty stomach, as certain foods and medications (i.e iron) may interfere with absorption of levothyroxine. Use caution when administering levothyroxine together with calcium supplements. The calcium will interfere with the absorption of levothyroxine as well. Take any products containing calcium at least four hours before or after taking levothyroxine.
*Note that during initial therapy the most common adverse reaction is signs of hyperthyroidism, indicating overdose.
*Note that early effects are noted within 48 hours. It may take up to several weeks of therapy to notice a complete therapeutic response.
Thyroid replacement therapy such as levothyroxine (Synthroid) or liothyronine sodium (Cytomel) are oral drugs. Low dose is started and then increased or decreased until therapeutic level is reached. See Drug Therapy Table 50-1 in Timby & Smith page 762 for additional drugs used. Drugs may be required for lifetime depending on underlying cause.
The drug of choice to treat hypothyroidism is levothyroxine (Synthroid) because it is relatively inexpensive, dosed at once a day, has more uniform potency than others. For this reason it is important to educate patients not to switch to another brand(generic) unless physican has reviewed. Not all thyroid hormone replacement drugs are equivalent. It is also important to take levothyroxine in the morning on an empty stomach, as certain foods and medications (i.e iron) may interfere with absorption of levothyroxine. Use caution when administering levothyroxine together with calcium supplements. The calcium will interfere with the absorption of levothyroxine as well. Take any products containing calcium at least four hours before or after taking levothyroxine.
*Note that during initial therapy the most common adverse reaction is signs of hyperthyroidism, indicating overdose.
*Note that early effects are noted within 48 hours. It may take up to several weeks of therapy to notice a complete therapeutic response.
Source: NEC
Memory Notebooks
Nursing Management
•Monitor VS
•Monitor for cardiac complications
•Thyroid replacement therapy
–Administer and monitor thyroid replacement of dessicated thyroid, thyroxine (Synthroid), triiodothyronine (Cytomel) as prescribed
–Monitor for S&S of hyperthyroidism from medication therapy. Could indicate overdose.
•Monitor for overdose of thyroid meds – tachycardia, restlessness, nervousness, and insomnia
•Instruct client in low-calorie, low-cholesterol, low-saturated fat diet
•Monitor for anorexia and constipation – prevent constipation by gradually increasing exercise, administering stool softeners, increasing bulk in diet, promoting regular bowel habits. Avoid enemas DT vagal stimulation.
•Provide a warm environment for client
•Avoid sedatives and narcotics due to intolerance – if must be given, give lowest dose and monitor mental status, level of consciousness, and respirations
•Teach pt nature of thyroid hormone deficiency, self-care practices necessary to recover, and S&S to monitor
•Energy level and mental alertness should be noted.
See "Nursing Process for the Client with Hypothyroidism" Ch. 50 p. 767
•Monitor VS
•Monitor for cardiac complications
•Thyroid replacement therapy
–Administer and monitor thyroid replacement of dessicated thyroid, thyroxine (Synthroid), triiodothyronine (Cytomel) as prescribed
–Monitor for S&S of hyperthyroidism from medication therapy. Could indicate overdose.
•Monitor for overdose of thyroid meds – tachycardia, restlessness, nervousness, and insomnia
•Instruct client in low-calorie, low-cholesterol, low-saturated fat diet
•Monitor for anorexia and constipation – prevent constipation by gradually increasing exercise, administering stool softeners, increasing bulk in diet, promoting regular bowel habits. Avoid enemas DT vagal stimulation.
•Provide a warm environment for client
•Avoid sedatives and narcotics due to intolerance – if must be given, give lowest dose and monitor mental status, level of consciousness, and respirations
•Teach pt nature of thyroid hormone deficiency, self-care practices necessary to recover, and S&S to monitor
•Energy level and mental alertness should be noted.
See "Nursing Process for the Client with Hypothyroidism" Ch. 50 p. 767
Cretinism
Cretinism
– hypothyroidism in infancy (1 in 4000-5000 newborns – rare in US)
•Caused by thyroid hormone deficiencies during fetal or early neonatal life.
•May be due to maternal iodine deprivation or congenital thyroid abnormalities
•Major manifestations of cretinism are irreversible defective physical development (dwarfism) and mental retardation.
•May appear normal at birth, but should be expected when there is a long gestational period and failure to thrive.
• Also called Congenital hypothyroidism
Typical physical characteristics include:
S&S:
Treatment:
Consists of hormone replacement which then allows for progression of normal physical and intellectual development.
•Similar to hypothyroidism.
•Soft diet, if gland markedly enlarged or if client has difficulty swallowing
– hypothyroidism in infancy (1 in 4000-5000 newborns – rare in US)
•Caused by thyroid hormone deficiencies during fetal or early neonatal life.
•May be due to maternal iodine deprivation or congenital thyroid abnormalities
•Major manifestations of cretinism are irreversible defective physical development (dwarfism) and mental retardation.
•May appear normal at birth, but should be expected when there is a long gestational period and failure to thrive.
• Also called Congenital hypothyroidism
Typical physical characteristics include:
- USUALLY SEVERELY MENTALLY RETARDED
- SHORT STATURE
- SHORT LIMBS
- BROAD NOSE
- THICK TONGUE
- PUFFY EYELIDS
- IF TREATED ASAP, MAY RESULT IN NORMAL DEVELOPMENT
S&S:
- exhibit squinting
- excessive sleeping
- thickened skin and lips
- enlarged tongue
- hoarse cry
- dull facial expression
- respiratory difficulty
- supraclavicular and
- periorbital edema
- umbilical hernia
- hypothermia
Treatment:
Consists of hormone replacement which then allows for progression of normal physical and intellectual development.
•Similar to hypothyroidism.
•Soft diet, if gland markedly enlarged or if client has difficulty swallowing

Source: Unknown
Juvenile hypothyroidism
Juvenile hypothyroidism
- Has causes similar to those in adults.
- Requires prompt diagnosis and treatment to prevent developmental retardation.
- Usually due to autoimmune thyroiditis
- Intellectual development is normal, but physical and sexual development is altered.
- Face remains childlike, eruption of permanent teeth and sexual maturation is delayed
Myxedema
- Most severe form of hypothyroiditis
- Occurs in severe, long-standing hypothyroidism
- Typical in women over 50 yrs
- When untreated and advanced can lead to myxedemic coma
-
The term myxedema is often used
interchangeably with hypothyroidism.
•slowing of body processes
•personality changes
•mental impairment
•fatigue
•constipation
•weight gain
•menstrual changes
•dry skin
•cold intolerance
•coarse / hair loss
•hoarseness, low pitched voice
•myalgias
•goiter
•cardiac disorders
•reflex delay
•hypothermia
•hypotension
•hypoventilation
•ataxia
Unless hypothyroidism occurs after thyroidectomy or during treatment with antithyroid drugs, the symptoms may occur over months to years.
*Note that in adults, hypothyroidism is characterized by slowing of body processes.
Medical and Nursing Management
•Monitor VS
•Monitor for cardiac complications
•Thyroid replacement therapy
–Administer and monitor thyroid replacement of dessicated thyroid, thyroxine (Synthroid), triiodothyronine (Cytomel) as prescribed
–Monitor for S&S of hyperthyroidism from medication therapy. Could indicate overdose.
•Monitor for overdose of thyroid meds – tachycardia, restlessness, nervousness, and insomnia
•Instruct client in low-calorie, low-cholesterol, low-saturated fat diet
•Monitor for anorexia and constipation – prevent constipation by gradually increasing exercise, administering stool softeners, increasing bulk in diet, promoting regular bowel habits. Avoid enemas DT vagal stimulation.
•Provide a warm environment for client
•Avoid sedatives and narcotics due to intolerance – if must be given, give lowest dose and monitor mental status, level of consciousness, and respirations
•Teach pt nature of thyroid hormone deficiency, self-care practices necessary to recover, and S&S to monitor
•Energy level and mental alertness should be noted
Thyroiditis (Hashimoto's)
- An inflammation of the thyroid gland, which can be classified as acute, subacute, or chronic.
- Thyroid becomes enlarged from the inflammation, becomes tender in some cases.
- Excess thyroid hormone is released from stores within the thyroid gland not pituitary so creates hypermetabolic state. Once the stores of thyroid hormone deplete, the body enters a hypometabolic state which may become permanent in some cases, although in other cases, the thyroid does recover.
- Autoimmune response causes antibodies that destroy thyroid tissue to develop.
- Functional thyroid tissue is replaced with fibrous tissue, and TH levels decrease…this prompts gland to enlarge and compensate, causing a goiter.
- This disorder is more common in women – the most common cause of goiterous hypothyroidism is the US.
- Can be treated, but not cured.
Types:
- Acute thyroiditis occurs in children usually due to bacterial infection of the gland. Usually is rare due to efficacy of antibiotics.
- Subacute thyroiditis can result after an upper respiratory infection, while a second type may result from autoimmune response, usually occurring in the post-partum period.
- Chronic thyroiditis (Hashimoto's thyroiditis), a common type, is thought to be caused by an autoimmune response.
Data collection
–enlarged thyroid gland, lumpy surface
–possible dysphagia (implies speech due to speech area injury in brain)
–feeling of fullness
–other sx similar to hypothyroidism
– radioactive iodine shows increase in iodine uptake
Implementation
•Similar to hypothyroidism
•Soft diet, if gland markedly enlarged or if client has difficulty swallowing
•Thyroid replacement therapy
–enlarged thyroid gland, lumpy surface
–possible dysphagia (implies speech due to speech area injury in brain)
–feeling of fullness
–other sx similar to hypothyroidism
– radioactive iodine shows increase in iodine uptake
Implementation
•Similar to hypothyroidism
•Soft diet, if gland markedly enlarged or if client has difficulty swallowing
•Thyroid replacement therapy
Example of goiters (figure 50-6 p. 770)
Timby & Smith, 2013
Lippincott Williams & Wilkins
