Treatment of type I DM involves a team consisting of the patient, caregivers, health care practitioner, nurse, nutritionist, and mental health professional (Potts & Mandleco, 2007).
General goals for the patient are to achieve normal growth and development (in children), optimal glucose managment, minimal complications, and a positive adjustment to the disease (Potts & Mandleco, 2007; Timby & Smith, 2013).
Medical treatment will include daily injections of insulin, blood glucose monitoring and management, following a meal plan, exercise, self-management skills. For patients with Type II DM, oral hypoglycemics may be utilized to supplement therapy.
General goals for the patient are to achieve normal growth and development (in children), optimal glucose managment, minimal complications, and a positive adjustment to the disease (Potts & Mandleco, 2007; Timby & Smith, 2013).
Medical treatment will include daily injections of insulin, blood glucose monitoring and management, following a meal plan, exercise, self-management skills. For patients with Type II DM, oral hypoglycemics may be utilized to supplement therapy.

A. Pre-filled Insulin Pens
|

B. Regular and NPH insulin in multi-dose vials.
|

C. Insulin pump
|
Insulin management therapy may include the use of various types of insulins.
Insulin is administered by subcutaneous injections (figure A, B) or a portable insulin pump (figure C). The frequency of the injections will vary according to the prescribed treatment and the goals of management for the client. It is not uncommon to have two or three daily injections in a client with type I DM. An increasing trend among children and teenagers is the insulin pump (C). The insulin pump provides the child or teen with a more discrete and manageable method of controlling their condition. Current pumps are approximately the size of a pager and contain a syringe that can hold up to 300 units of insulin (Potts & Mandleco, 2007). The pump works by delivering insulin via a tiny catheter that is placed every 2 to 3 days into subcutaneous fat. The pump is programmed to deliver the insulin continuously throughout the day and night, in small amounts. An immediate bolus of insulin is programmed to be delivered with each snack and meal. This bolus is based on the dose of insulin that is essential for the carbohydrate consumption and the individual's blood glucose level. Several studies have shown that pump therapy reduces episodes of severe hypoglycemia in pediatric populations as well as increases client satisfaction (Potts & Mandleco, 2007).
More information about insulin pumps available at http://www.diabetes.org/living-with-diabetes/treatment-and-care/medication/insulin/insulin-pumps.html.
The most commonly used insulin is synthetic human, which is produced through recombinant DNA technology (Potts & Mandleco, 2007).
The dosage of insulin is based on the needs of the client. Common dosage for a child "more than one year postdiagnosis is 0.75-1.0 units/kg/day". The insulin needs in the adolescent tend to "exceed 1.0 units/kg/day, and may sometimes reach up to 1.6-1.7 units/kg/day" (Potts & Mandleco, 2007, p. 903).
Some insulins may be mixed together but there are others that are not safe to mix. Example: Regular insulin may be mixed with Lispro insulin=stable when mixed with Lente and NPH. However Lente and Ultra Lente are unstable if mixed with NPH. Lantus cannot be mixed with any other insulin in the same syringe. It must be administered in its own syringe.
Insulin is administered by subcutaneous injections (figure A, B) or a portable insulin pump (figure C). The frequency of the injections will vary according to the prescribed treatment and the goals of management for the client. It is not uncommon to have two or three daily injections in a client with type I DM. An increasing trend among children and teenagers is the insulin pump (C). The insulin pump provides the child or teen with a more discrete and manageable method of controlling their condition. Current pumps are approximately the size of a pager and contain a syringe that can hold up to 300 units of insulin (Potts & Mandleco, 2007). The pump works by delivering insulin via a tiny catheter that is placed every 2 to 3 days into subcutaneous fat. The pump is programmed to deliver the insulin continuously throughout the day and night, in small amounts. An immediate bolus of insulin is programmed to be delivered with each snack and meal. This bolus is based on the dose of insulin that is essential for the carbohydrate consumption and the individual's blood glucose level. Several studies have shown that pump therapy reduces episodes of severe hypoglycemia in pediatric populations as well as increases client satisfaction (Potts & Mandleco, 2007).
More information about insulin pumps available at http://www.diabetes.org/living-with-diabetes/treatment-and-care/medication/insulin/insulin-pumps.html.
The most commonly used insulin is synthetic human, which is produced through recombinant DNA technology (Potts & Mandleco, 2007).
The dosage of insulin is based on the needs of the client. Common dosage for a child "more than one year postdiagnosis is 0.75-1.0 units/kg/day". The insulin needs in the adolescent tend to "exceed 1.0 units/kg/day, and may sometimes reach up to 1.6-1.7 units/kg/day" (Potts & Mandleco, 2007, p. 903).
Some insulins may be mixed together but there are others that are not safe to mix. Example: Regular insulin may be mixed with Lispro insulin=stable when mixed with Lente and NPH. However Lente and Ultra Lente are unstable if mixed with NPH. Lantus cannot be mixed with any other insulin in the same syringe. It must be administered in its own syringe.
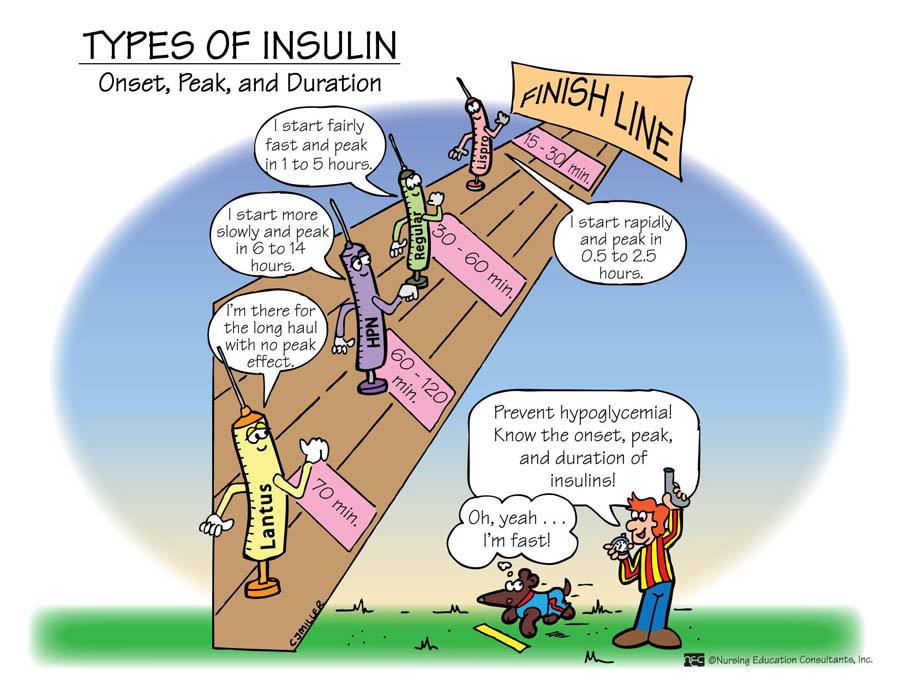
Types of Insulin Preparations and Action (Table 51-2)
|
Name
Lispro (Humalog) Aspart (Novolog) Regular (Humulin R, Novolin R) NPH Lente Ultralente, Humulin U Glargine (Lantus) Premixed 70/30 Premixed 75/25 |
Type
Rapid-Acting Rapid-Acting Short-Acting Intermediate-Acting Intermediate-Acting Long-acting Long-acting 70% NPH with 30% Regular or Novolog (mixture) 75% NPH with 25% (Humalog) |
Onset
5-15 min 5-15 min 30-60 min 1-1.5 hours 1-2.5 hours 4-8 hours 2-4 hours 30 min 15 minutes |
Peak
30-60 min 60 min 1-3 hours 4-12 hours 7-15 hours 8-10 hours No peak 7-12 hours 2 hours |
Duration
3-4 hours 3-4 hours 6-8 hours 24 hours 24 hours 18-30 hours = or >24 hours 16-24 hours 20-22 hours |
(Source: Timby & Smith, 2013, p. 789)
Source: NEC Memory Notebooks
Sites of Insulin Administration
It is important to instruct the patient and caregivers on the proper sites of administration for insulin injections. Insulin is administered into the subcutaneous fat which is found in the abdomen, back of the arms, legs, and above the buttocks. The abdomen has the fastest and most consistent absorption rate, followed by the arms. Insulin injections are absorbed the slowest in the legs and buttock sites. If proper site selection and rotation are not utilized, the individual receiving the injections may suffer from lipoatrophy (indentation or atrophy of subcutaneous fat) or lipohypertrophy (lumpiness or hypertrophy of subcutaneous fat) specifically at the sites of injection (Potts & Mandleco, 2007). Therefore for this reason the mechanics of rotating sites with each injection should be taught to the patient and caregivers administering the injections. They need to understand the complications that arise from lipoatrophy and lipohypertrophy. Lipoatrophy is uncommon today with the use of purified insulin preparations available and is "treated by injecting insulin into the edges of the area of atrophy" (Potts & Mandleco, 2007, p. 907). Lipohypertrophy occurs more commonly and is a result of trauma to the injection sites from repeated injections to the same area. It results in a cosmetically unsightly area that has decreased sensation and absorption. Lipohypertrophy resolves by avoiding the area for injections (Potts & Mandleco, 2007).
|
Sites of subcutaneous administration
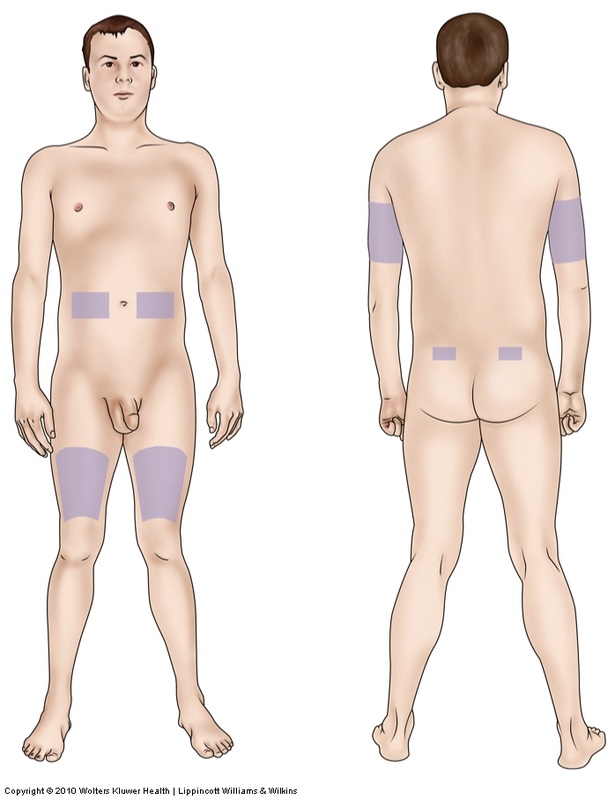
Source: Timby & Smith, 2013, p. 790
Lippincott, Williams & Wilkins
|
Complications of site overuse

Lipohypertrophy
Source: www.nejm.org/doi/full/10.1056/NEJMicm1101527
|
Oral antidiabetic agents
Oral medications for Type II DM help to supplement therapy. The patient must meet specific criteria in order to be prescribed oral medication.
There are various types of oral medications now available. See chart below for names.
- They must have fasting glucose level < 200 mg/dL
- Insulin requirements of less than 40 units/day
- No ketoacidosis
- No kidney or liver disease
There are various types of oral medications now available. See chart below for names.
|
The oldest category are the sulfonylureas. They derive from sulfa antibiotics. Sulfonylureas help to stimulate the pancreas to secrete more insulin. They are known as "insulin releasers" (Timby & Smith, 2013, p. 791). The first-generation sulfonylureas are not commonly used today due to their long duration of action and higher incidence of adverse reactions, as well as interactions with other drugs. Examples of 1st generation sulfonylureas are acetohexamide, chlorpropamide (Diabinese), tolazamide (Tolinase), and tolbutamide (Roach & Ford, 2010, p. 422).
More commonly used 2nd generation Examples: glyburide (DiaBeta, Glynase, Micronase); glimepride (Amaryl), glipizide (Glucotrol) SE: weight gain, hypoglycemic reactions and secondary failure, meaning the pancreas stops making enough insulin, perhaps due to overstimulation, anorexia, nausea, vomiting, heartburn, diarrhea, allergic reactions, CV mortality. WARNING: do not take if allergic to sulfa drugs or if pregnant. Do not mix with alcohol. Meglitinides such as repaglinide (Prandin) are also used to help stimulate the pancrease to produce more insulin.
SE: upper respiratory infections, hypoglycemia, headache, hyperglycemia Monitor urine and serum glucose levels Teach patient The next category of oral antidiabetics are the "insulin sensitizers", the Biguanides and Thiazolinades (TZDs). These medications help tissues to use the available insulin more efficiently (p. 792).
Examples: Metformin (Glucophage) is the only biguanide approved for use. SE: no weight gain, anorexia, nausea, heartburn, diarrhea, lactic acidosis, hypoglycemia, allergic skin reaction, flatulence. WARNING: Avoid in pregnancy, avoid taking with alcohol, do not discontinue abruptly. TZDs: rosiglitazone (Avandia), pioglitazone (Actos) SE: weight gain, edema, liver damage, headache, pain, infections, fatigue, risk for heart attack or heart failure WARNING: Monitor liver function, monitor for weight gain, edema- indicates HF |
Alpha-Glucosidase Inhibitors
These drugs slow the process of forming glucose by preventing the breakdown of complex to simple carbs which normally occurs with the intestinal enzyme alpha-glucosidase. By slowing this process down, it also slows the absorption of glucose in the small intestine. These drugs are to be taken 15 minutes prior to each meal. Can be taken by patients with Type I DM to help balance post-prandial glucose to prevent fluctuations of hyper and hypoglycemia. Gives better control. Examples: Acarbose (Precose), miglitol (Glyset) WARNING: If hypoglycemia is experienced after taking this drug, fruit juice cannot be used to treat. Drug prevents conversion of fructose to glucose. Must give glucose tablets or glucagon since no conversion is needed with these. Adjuvant Drugs
These drugs are based on hormones with glucose-regulating functions. They are used in adjunct with other traditional drugs to potentiate the effect of managing diabetes better. These drugs mimic hormones such as amylin (found in pancreas), incretin (found in intestines), which normally lower blood sugar and promote secretion of insulin, respectively, thus improving metabolism of carbs (Timby & Smith, 2013, p. 792-793). Benefit of therapy with these drugs is that blood sugar is regulated more effectively and result in weight loss. Disadvantages: require multiple daily injections, although a long-acting injection is in the works. Examples: Pramlintide (Symlin) and exenatide (Byetta) Dipeptidyl peptidase IV (DPP-4) Inhibitor Sitagliptin (Januvia) is an oral drug and works similarly to pramlintide, except it helps to block the breakdown of amylin. Januvia should serve as an adjunct drug, not used alone. There has recently been a new drug approved by the FDA, Janumet, a combination of sitagliptin and metformin in one pill (Timby & Smith, 2013, p. 792). WARNING: Do not use with Type I DM; assess renal function and continue to monitor. Do not start if renal dysfunction; assess glucose levels for efficacy |
| Diabetes Mellitus Medication Therapy 2013 |
Pancreas Transplantation
Read on your own page 794
Read on your own page 794
Islet Cell Transplantation
Read on your own page 794
Read on your own page 794
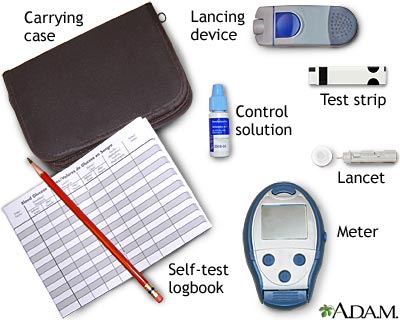
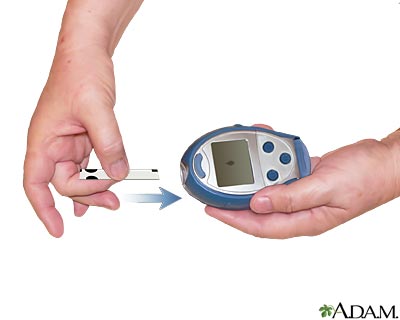
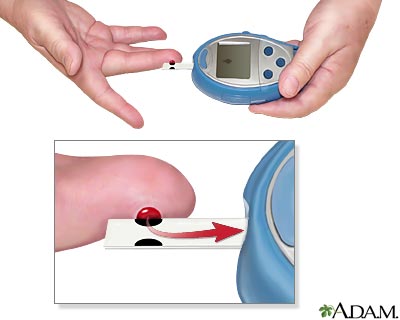
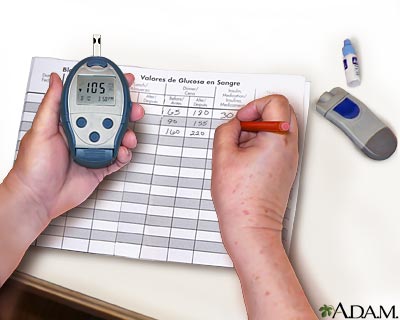
Blood Glucose Monitoring
Monitoring blood glucose levels is essential to proper management of type I diabetes. Home blood glucose monitoring is available for convenience and facilitation of self-management. Glucose monitoring at home consists of lancing the fingertip or other appropriate area (new meters are able to test small blood samples from the forearm, thigh, or side of hand) (Potts & Mandleco, 2007). The blood sample is then placed on a testing strip in the glucose meter. The glucose level is then measured by the meter. Frequency of glucose testing is determined upon the goals of the individual's management.
|
|
|
|
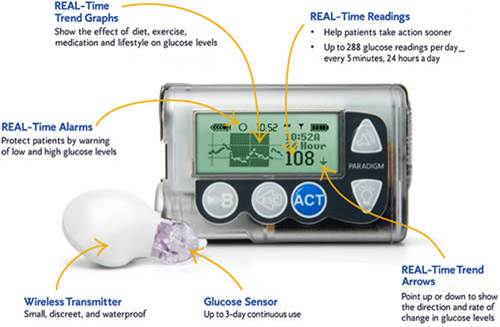
Continuous glucose monitoring
- Sensor is inserted subcutaneously
Evaluation for a 24 hour period
|

|
Medical Monitoring Recommendations
Medical monitoring is essential to meet the ongoing needs of the child with type I diabetes. The individual is monitored for immediate, intermediate, and long-term complications.
*Semi-annual or quarterly exams
*Height measurement (until maturity)
*Weight
*Blood pressure (quarterly)
*Sexual maturity staging (periodically in the peripubertal client)
*Foot exam with quarterly exam
*Comprehensive eye examination for all individuals over age 10 after 3-5 years of diagnosis
*Medical history: include frequency or severity of hypoglycemia, home blood glucose monitoring (HBGM) results, regimen adjustments made by client lifestyle changes, symptoms of complications, medications, psychosocial issues
*Annual physical exam (any abnormality noted is reevaluated at next visit)
*Laboratory evaluation: Hemoglobin A1c is 2-4 times per year, fasting lipid panel at time of diagnosis, then every 5 years unless positive risk factors, annual urine screening for microalbumin after 5 years of diagnosis, and older than 10 years.
*Review of management plan- each encounter
(Potts and Mandleco, 2007, p. 904)
*Height measurement (until maturity)
*Weight
*Blood pressure (quarterly)
*Sexual maturity staging (periodically in the peripubertal client)
*Foot exam with quarterly exam
*Comprehensive eye examination for all individuals over age 10 after 3-5 years of diagnosis
*Medical history: include frequency or severity of hypoglycemia, home blood glucose monitoring (HBGM) results, regimen adjustments made by client lifestyle changes, symptoms of complications, medications, psychosocial issues
*Annual physical exam (any abnormality noted is reevaluated at next visit)
*Laboratory evaluation: Hemoglobin A1c is 2-4 times per year, fasting lipid panel at time of diagnosis, then every 5 years unless positive risk factors, annual urine screening for microalbumin after 5 years of diagnosis, and older than 10 years.
*Review of management plan- each encounter
(Potts and Mandleco, 2007, p. 904)
Nutrition
Nutrition is very important in the individual with diabetes. A meal plan specific to the individual's goals and needs should be developed. There is no longer exclusion of certain foods, i.e candy, pie, sweets in general. Now, a typical meal plan will provide balanced nutrition such as grains, breads, fruit, vegetables, and meats, beans, eggs, cheese, and legumes. Individuals may even allow some fats into their diet. The breakdown of food groups is 50-60% of the calories derived from carbohydrates, 10-20% from protein, and 20-30% from fats. In order to be successful in dietary management, the individual must be encouraged to set realistic and specific goals that can be met (Potts & Mandleco, 2007). Using the glycemic index is recommended to help maintain normal glucose levels low. The glycemic index is a measure of how fast a carbohydrate food is likely to raise blood sugar (Timby & Smith, 2013, p. 788). Foods with indices greater than 70 are likely to raise low blood sugar faster and are best used to cover brief periods of intense exercise. Foods lower than 55, (i.e. low fat yogurt), are used to slowly prevent hypoglycemia during night or long periods of rest (p. 788).
Exercise
Physical activity plays an important role in the management of diabetes "as it potentiates the hypoglycemic effect of insulin" (Potts & Mandleco, 2007, p. 905). Increasing physical activities such as exercise (walking, running, jogging) assists in decreasing blood glucose levels and improves glucose control. For instance, some individuals with higher levels of activity may be allowed a larger meal plan or lower doses of insulin. It is vital to adequately prepare for the changes that exercise may produce. Insulin dosages will need to be changed as well as diet. Recall that exercise helps to stimulate the transporter proteins in skeletal muscles to allow for more glucose to enter the cell.
Hypoglycemia
Hypoglycemia is a complication of diabetes. It is also called an insulin reaction or low blood glucose. Hypoglycemia occurs when the blood glucose levels drop below 60 mg/dL. The cause is when more insulin is available than is necessary and may be a result from an insulin overdose, insufficient food consumption, or increased activity (Potts & Mandleco, 2007).
Symptoms of mild to moderate hypoglycemia may include
*Drowsiness
*Lightheadedness/dizzy
*Irritability
*Tremors
*Sweating/diaphoretic
*Pallor
*Confusion/poor concentration
*Feeling strange
*Hungry
*Rapid heart beat
*Numbness or tingling around mouth or tongue
*****Severe hypoglycemia symptoms (rare) may lead to unconsciousness and convulsions and can be life-threatening if not treated promptly (Potts & Mandleco, 2007).
***Note that diaphoresis is a clinical feature that distinguishes hypoglycemic reaction from a ketoacidosis reaction.
Treatment
For mild hypoglycemia may include:
Eating a food that contains 15 grams of a fast-acting carbohydrate (sugar)
1/2 cup of juice or regular soda
5 sugar cubes
1 small box of raisins
6-7 hard candies (not sugar free)
3 glucose tablets (5 grams of glucose each)
8 oz. skim milk
Patients should be instructed to always carry a quick-acting carbohydrate in their purse or pocket, even in their vehicle. After administration or consumption of any food listed above, wait 15 minutes and recheck the blood glucose levels. May repeat if necessary. If the next meal is more than an hour away, may eat one of the following: 1 peanut butter sandwich, cheese and crackers, or drink 1 cup of skim milk (Texas Diabetes Council, 2007).
Moderate hypoglycemia treatment may include 10-15 grams of a carbohydrate but will also require some medical assistance.
Severe episodes of hypoglycemia require IV glucose or IM glucagon. Treatment options, glucagon preparation and administration of IM glucagon should be taught to the caregivers. Medical assistance is required for administration of IV glucose and other measures to prevent further complications.
Symptoms of mild to moderate hypoglycemia may include
*Drowsiness
*Lightheadedness/dizzy
*Irritability
*Tremors
*Sweating/diaphoretic
*Pallor
*Confusion/poor concentration
*Feeling strange
*Hungry
*Rapid heart beat
*Numbness or tingling around mouth or tongue
*****Severe hypoglycemia symptoms (rare) may lead to unconsciousness and convulsions and can be life-threatening if not treated promptly (Potts & Mandleco, 2007).
***Note that diaphoresis is a clinical feature that distinguishes hypoglycemic reaction from a ketoacidosis reaction.
Treatment
For mild hypoglycemia may include:
Eating a food that contains 15 grams of a fast-acting carbohydrate (sugar)
1/2 cup of juice or regular soda
5 sugar cubes
1 small box of raisins
6-7 hard candies (not sugar free)
3 glucose tablets (5 grams of glucose each)
8 oz. skim milk
Patients should be instructed to always carry a quick-acting carbohydrate in their purse or pocket, even in their vehicle. After administration or consumption of any food listed above, wait 15 minutes and recheck the blood glucose levels. May repeat if necessary. If the next meal is more than an hour away, may eat one of the following: 1 peanut butter sandwich, cheese and crackers, or drink 1 cup of skim milk (Texas Diabetes Council, 2007).
Moderate hypoglycemia treatment may include 10-15 grams of a carbohydrate but will also require some medical assistance.
Severe episodes of hypoglycemia require IV glucose or IM glucagon. Treatment options, glucagon preparation and administration of IM glucagon should be taught to the caregivers. Medical assistance is required for administration of IV glucose and other measures to prevent further complications.
Glucagon Kit with Instructions

Glucagon Kit
Source:
http://www.diabetesmine.com/2011/08/ask-dmine-type-1-kids-and-birthday-parties-how-glucagon-works.html
|

Source:
http://www.healthcentral.com/diabetes/h/effect-of-glucagon-hypersecretion.html
|
Treating hypoglycemia at home
Recognizing symptoms of Hypoglycemia
Video References:
Children's Hospital
Children's Hospital
